Criteria for Gamma Probe Systems
1. Overview
Regardless of all technical details are "Crystal Probe" gamma detection systems in all configurations best suited for Sentinel Surgery according to the official guidelines of the German Society of Senology and the German Society of Nuclear Medicine.
Most commercially available gamma probe systems follow a very similar technical concept: a small detection probe connected to a portable control unit. Sometimes it is claimed to have the most sensitive probe, hence best performance, but there are some more important criteria next to sensitivity that must be met too for an overall optimal performance.
The following performance indicators are considered to be most essential (WENGENMAIR et.al., KLINIKUM AUGSBURG):
| Performance Criteria | Medical Demand | Crystal Probe -automatic- |
| Sensitivity | > 5,000 cps/MBq | > 20,000 cps/MBq |
| Angular Resolution | < 40° FWHM | < 40° FWHM |
| Spatial Resolution | < 25 mm FWHM | < 17mm FWHM |
| Side Shielding | > 99.9% | > 99.97% |
In this section we discuss these criteria, which only combined result in optimal performance, along with the performance of our Crystal Gamma Probe.
- Sufficient sensitivity: Highly sensitive detector results in faster procedures and/or less nuclide injection hence radioactive contamination
- Radial sensitivity: Background signal should be much lower than the target signal
- Spatial resolution: For precise localization of the sentinel lymph node
- Proper side-shielding: Eliminates scatter radiation from the side and back of the probe
- Good energy resolution: Separates scatter radiation from photopeak signal
- Clear display of signal: Both visual and acoustic signalisation without delay
2. Sensitivity

The sensitivity E of the probe is determined directly at the tip of the probe or collimator: The probe is placed in a fixed distance directly above a gamma emitter with well known activity A (Mbq or µCi), then the measured signal S (cps=counts per second) is related to this activity: E=S/A.
In general the necessary sensitivity depends on radionuclide uptake, measurement geometry and time between injection and SLNE. The maximum radionuclide uptake of the sentinel lymph node typically varies between 0.01% and 1% with a median at around 0.1%. The SLNE is mostly performed at the day after 99mTc -Nanocolloid injection. Then about 0.05% to 0.005% of the administered activity can be found in the lymph node intraoperatively. Assuming a typical activity application of 80 MBq a spot of activity between 4 and 40 kBq has to be localized. The sensitivity of the measurement system therefore should be better than 5 cps/kBq.
Performance of the Crystal Probe
The Crystal Probe’s sensitivity measures at >20,000 cps/MBq. Optimal results demand a minimum sensitivity of >5,000 cps/MBq. The sensitivity of a probe is very important. The more sensitive the probe, the easier it is to find the sentinel lymph node. Also, a higher sensitive probe will result in injecting less radioactive fluid into the patient. The Crystal Probe is four times more sensitive than required.
3. Radial Sensitivity
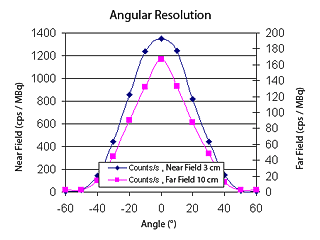
The sensitivity distribution is evaluated equidistant to the frontal radiation entrance window dependent on the polar angle. The full width at half maximum (FWHM) of the distribution function is a good quality criterion for the detectability of lymph nodes in presence of non target radiation (injection depot, background). With a broad measurement cone the background signal can exceed the target signal of the lymph node, which then cannot be detected. A small cone mainly reduces background maintaining a constant target signal. Therefore with increased background in the target area a smaller FWHM of radial sensitivity distribution is desired.
Performance of the Crystal Probe
The Crystal Probe’s measured far distance Field of View (FOV) is <40° FWHM, exactly in the appropriate range for optimal radial sensitivity distribution. Radial sensitivity is essential in pinpointing the exact lymph node (the sentinel lymph node, SLN). A larger FOV may include two nodes which is unnecessary and a smaller FOV makes it difficult to find the SLN (because the sensitivity is smaller, if the SLN is not completely within the FOV), which wastes time.
And additionally: For different approaches intraoperatively it is possible, to exchange collimators with different FOV, thus switching between high overall detection in the beginning and then changing to high local sensitivity searching in a small area. For this purpose we offer a variation of collimators with different FOV.
4. Spatial Resolution
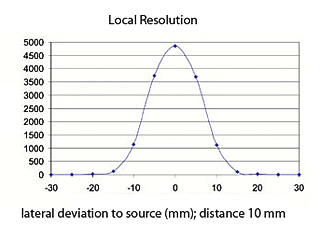
The spatial resolution can be determined if a surgical gamma probe is scanned laterally above a radioactive point source.
Spatial resolution depends on the distance between source and probe detector. To separate neighbouring lymph nodes and perform an adequate exact localization, the FWHM (Full Width at Half Maximum) of the lateral sensitivity distribution should be better than the typical distance between neighbouring lymph nodes or a typical node diameter in the preparation region. Therefore a spatial resolution better than 25 mm for lymph nodes in the axilla, inguinal and illiacal region is ideal. Increased requirements have to be set up for lymph nodes that are close together (e.g., in the head, neck and supraclavicular region). Probes for these applications should have a FWHM of less than 15mm.
Performance of the Crystal Probe
The Crystal Probe’s spatial resolution measures at <17mm FWHM at 1cm distance with a standard (40 °) collimator. Optimal results demand a local resolution of <25mm. The Crystal Probe exceeds the optimal result criteria. This good spatial resolution is fundamentally essential for locating the sentinel lymph node. Anything larger than the recommended 25mm FWHM will result in the removal of more than one node, or the wrong node.
5. Side-shielding
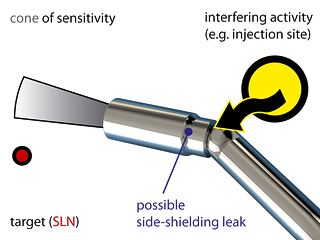
Due to constructional reasons, the shielding of a surgical gamma probe is mostly a weak area because it can only be improved by higher material thickness. A high background source (e.g. even the primary injection spot at a mammal or prostate carcinoma) in the direction of such a leakage can lead to false positive signals and orientation. The lymph node should produce a higher signal than any background source. Assuming an uptake of 0.1% for a lymph node the leak sensitivity should not exceed 0.1% of the system sensitivity.
Performance of the Crystal Probe
The Crystal Probe tungsten detector sleeve has a superior property of >99.97% shielding. The industry standard is determined at >99.9%.
6. Energy Resolution

With the presence of scatter if gamma photons travel through dense material, these scattered Compton photons have changed their energy and direction, thus producing an additional blurring of the spatial information. An energy discrimination that separates Compton and directly detected photopeak signals is therefore important.
Performance of the Crystal Probe
The Crystal Probe’s energy resolution is one of the best on the market. This is obtained by using not only a simple low energy discrimination, but also a second discrimination of higher energy photons originating from other nuclides or background radiation with any unknown origin. Good energy resolution is one of the most important requirements to consider. When the patient is injected with radioactivity, Technetium 99 for example, in order to identify the sentinel lymph node, the probe should detect Technetium 99 photopeak signal only and not scatter radiation or activity of any other origin. But with Crystal Probe -automatic- it is very easy to change the selection to another radionuclide, choosing from a table which is internally stored in the micro processor.
7. Display

All kinds of display have to be adapted to the special situation in an operation room. An acoustic signal should enable the user to visually concentrate to the operation field during measurement. Therefore a clear correlation between the acoustic tone and the measurement signal has to be available. For the quantitative results either a digital or analogue display is necessary which has to be clearly readable from at least 6 ft distance. To cope with the statistical variation and to influence the inertia of the display measurement interval respectively time constant should be adjustable.
Performance of the Crystal Probe
The Crystal Probes display illuminates the numerical counts which are easy to read. A bar graph displays a logarithmic analog. As a special feature the maximal count rate during the last 30 second period is displayed, to support protocol obligations. Build in routines for averaging the signal and to sum up counts ease usability. And there are several different clear, crisp acoustic signals to choose from.